 6501 Sprott St #1, Burnaby, BC V5B 3B8, Canada
6501 Sprott St #1, Burnaby, BC V5B 3B8, Canada 604-294-3376
604-294-3376Originally posted at: http://www.theguardian.com/lifeandstyle/the-running-blog/2014/jul/22/running-problems-plantar-fasciitis-joggers-heel on 22nd July 2014
This is the third in the series of injury blogs – after shin splints and ITB friction syndrome – and it tackles something that can be resistant to treatment, particularly if it is not caught early.
So what is plantar fasciitis?
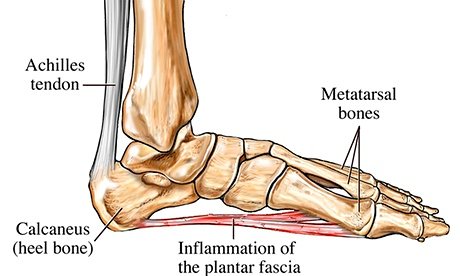
The plantar fascia is a thick band of connective tissue that runs along the underneath of the foot from the heel bone to the toes. At the heel it can also have fascial connections to the achilles tendon. Its job is to maintain the arch of the foot – it acts as a bowstring pulled between the heel and the toes. “Itis” as a suffix indicates inflammation, but with the plantar fascia there is still some controversy over what exactly happens to the tissue when it becomes painful.
What causes it?
This is a problem of either extreme, so people with high arches or those that have very flat feet are at risk of developing pain in this region. This is because of the relative stress the plantar fascia is put under. In people with excessive pronation, the plantar fascia is put under too much stretch, as their range flattens and strains it. People with a stiff, supinated (high-arched) foot lack the flexibility to appropriately shock absorb, so this too puts extra strain on the plantar fascia. Clinically, we see more people presenting with plantar fascia pain who have excessive pronation than those with stiff, supinated feet.
But while the foot type is the biggest risk factor for plantar fasciitis, the whole leg from the pelvis down can affect how the foot hits the ground. A thorough biomechanical assessment will determine where in the kinetic chain things have gone wrong to cause the overload.
Pain tends to start gradually, often just in the heel, but it can sometimes be felt along the whole of the plantar fascia. The symptoms are initially worse in the morning and mostly after, rather than during, activity. As the condition becomes worse, the symptoms become more persistent.
How do I treat it?
Treatment initially involves offloading the plantar fascia by:
• Avoiding aggravating factors – such as running.
• Taping – this can work very well to alleviate pain, and can be almost immediate. It isn’t a long-term solution, but can relieve symptoms in the beginning.
• Using a night splint to stretch the calf, so that less load is placed on the plantar fascia (if tightness in the calf is a factor).
• Using a gel heel cup – this can act to increase shock absorption, and by raising the heel there is also less stretch on the calf. So, temporarily, this may relieve pain in someone who has a tight calf.
• Massage – but this depends if the plantarfascia is actually tight or just painful. If it is tight, then massage can temporarily relieve the pain, but if it is irritated then taping and corrective footwear is preferable.
The causes need to be identified, as correcting them will form part of the treatment, so there is not a recipe that will fit everybody. But these are the areas that need to be assessed:
• Training and footwear – did you alter the volume/intensity of your training? This may explain the onset of pain. The type of trainers you wear is also important. About 10 years ago, there was a drive to wear very cushioned, anti-pronation trainers. Pronation almost became a rude word, as if it were not a normal movement. Now the trend has gone the opposite way, and there are a lot of barefoot and minimal trainers on the market. The problem is that there is not a solution that fits everyone, and a lot of these trends are driven by manufacturers. Trainers need to be appropriate for your foot type, running style and purpose. A lot of patients who present with plantar fascia pain do end up needing to change their footwear.
• Lower limb biomechanics – the angulation of the leg in relation to the pelvis as you move, as well as the knee position, can affect how the foot is loaded. Frequently patients with plantar fascia pain will need to correct issues higher up in their kinetic chain.
• Foot type – someone with a very flat foot may need to see a podiatrist. Podiatrists specialise in custom-made orthotics that reduce the load though the plantar fasica.
Sometimes the initial offloading and correction of biomechanical and training issues does not alleviate symptoms, and then other treatments may be considered:
• Acupuncture – definitely not a first-line treatment, as it is very painful, but I have had quite good results when I have used it. It is also not a standalone treatment, as the causative factors do need to be addressed.
• Extracorporeal shockwave therapy – anecdotal evidence is good, but research into its effectiveness is controversial. There are not many risks, but it is also quite painful.
• Corticosteroid injection – this may be useful in the short-term, but must be combined with other treatments as above. There is also some concern that an injection is associated with an increased risk of rupture of the plantar fascia.
• Plantar fasciectomy – where a portion of the attachment close to the heel bone is removed. This is a last resort, and not one I would want to recommend.
So the take-home message is catch it early and offload. Don’t wait for the symptoms to become persistent, as it is a long journey back to running.
